When public hospitals purchase medical equipment or rely on outside doctors, they typically consider the price and quality of each vendor.
In Tarrant County, Texas, they consider something else, too: the race and gender of the vendor’s owners.
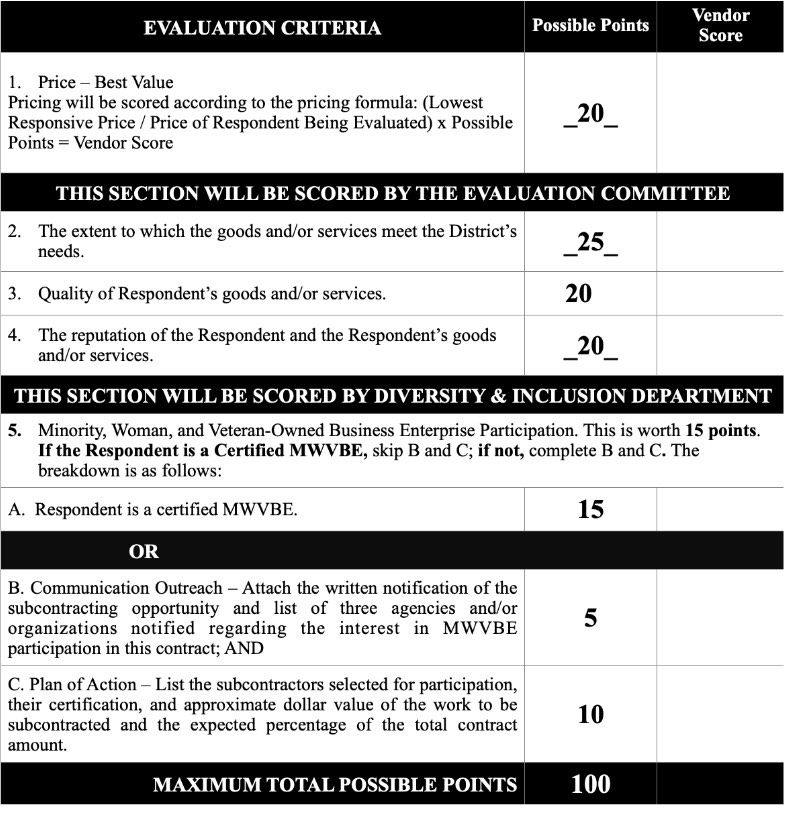
Tarrant County’s public hospital system, JPS Health, evaluates bids for contracts on a 100-point scale that gives more weight to “diversity and inclusion” (15 points) than to the reputation of a vendor’s goods and services (10 points) when assessing providers of transcatheter heart valves—devices used to counteract cardiac failure and keep blood flowing throughout the body.
It uses similar weights to select outside providers of cancer screenings. Price and quality receive 20 points each, according to a procurement request reviewed by the Washington Free Beacon, while diversity receives 15, enough to make up for major deficits in other areas. Minority-owned firms earn the 15 points automatically, the criteria state. Other firms are scored on their use of minority subcontractors, measured as a percent of the total contract value they receive.
JPS is just the latest health provider to integrate race into its procurement policies, balancing the cost and quality of life-saving services against the demographics of the firm providing them.
Inova Health System, the University of Virginia Medical Center, and the University of Texas MD Anderson Cancer Center have all issued requests for proposals that incorporate race. Others, such as Mount Sinai Health System, tout their record on “supplier diversity.”
The trend, critics say, which encompasses grant-making as well as contracting, threatens to undermine competent and cost-effective care in a country that already has the highest health care expenditures in the world. It comes amid a glut of diversity programs that have roiled the medical establishment, from affirmative action in medical schools to the allocation of COVID drugs based on race.
“The minority and other contracting preferences given by these hospitals tend to drive up prices and reduce the quality of goods and services,” said Judge Glock, the director of research at the Manhattan Institute, who has written at length about minority contracting. “The funds lost by the hospital could be used to treat needy people, as opposed to supporting less efficient but still successful businesses.”
The system means that public hospitals like JPS, which often rely on outside doctors for specialty services, are in some cases using race to decide who’s paid to diagnose cancer and other time-sensitive illnesses.
Tarrant County isn’t just seeking supplies like lab equipment, but also medical personnel to conduct blood tests, biopsies, and tissue analysis, per a procurement request for pathology services.
How well clinicians interpret those tests—which require advanced chemistry to understand—can mean the difference between catching a tumor early and letting it grow undetected. The criteria raise questions about how those clinicians are selected in a county that, according to JPS Health data, has higher rates of cancer than the state average and that is widely considered a Republican stronghold.
“They’ve thrown diversity into the mix where all they should be interested in is high quality service,” said Stanley Goldfarb, a professor of nephrology at the University of Pennsylvania medical school and the founder of the advocacy group Do No Harm. (Goldfarb is also the father of Free Beacon chairman Michael Goldfarb.) “Skimping on quality will result in missed diagnosis.”
JPS has posted dozens of requests for proposals since February that indicate race is used to evaluate bids. Though the weights for other factors vary across the requests, the 15 points for diversity do not.
Asked to comment on the scoring criteria, JPS claimed that it “does not consider ‘race’ or ethnicity as a basis for awarding contracts.” The health system “does gather that information,” a spokesperson wrote in an email, but “applies objective standards for determining the most qualified and best value vendors for the District.” JPS declined to answer follow-up questions about how the scoring sheets made their way into procurement requests.
Minority contracting is common, and costly, in industries such as construction, sanitation, and national defense. Government agencies have long set spending goals for “disadvantaged” firms—those in which women, veterans, or minorities hold a 51 percent stake—and targeted them with set-asides and no-bid contracts.
That practice has been linked to corruption and higher prices. One study found that Proposition 209, the California law that banned affirmative action in contracting, caused the cost of state highway projects to fall 5.6 percent relative to federal ones still subject to racial set-asides. Other research suggests that set-asides increase cost overruns and delays.
Now, as “health equity” becomes the watchword of hospital systems across the country, minority contracting has come for medicine. And it has led to some eyebrow-raising priorities, with fundamentals like price and quality taking a back seat to diversity.
The University of Virginia Medical Center said in 2019 that it would favor “Small, Woman-owned and Minority-owned” businesses when sourcing stem cell products. And in 2021, Inova Health gave race more weight than “cost-effectiveness” when evaluating applicants for its “Community Health Fund” grants, which support health care nonprofits in Northern Virginia working with “under-resourced communities.”
Inova, the largest health network in the area, gave 15 points to “BIPOC Owned/Led” organizations—the same amount as “overall impact” and “qualification and expertise”—but only 10 to budget considerations, according to Inova’s request for proposals document outlining the evaluation process.
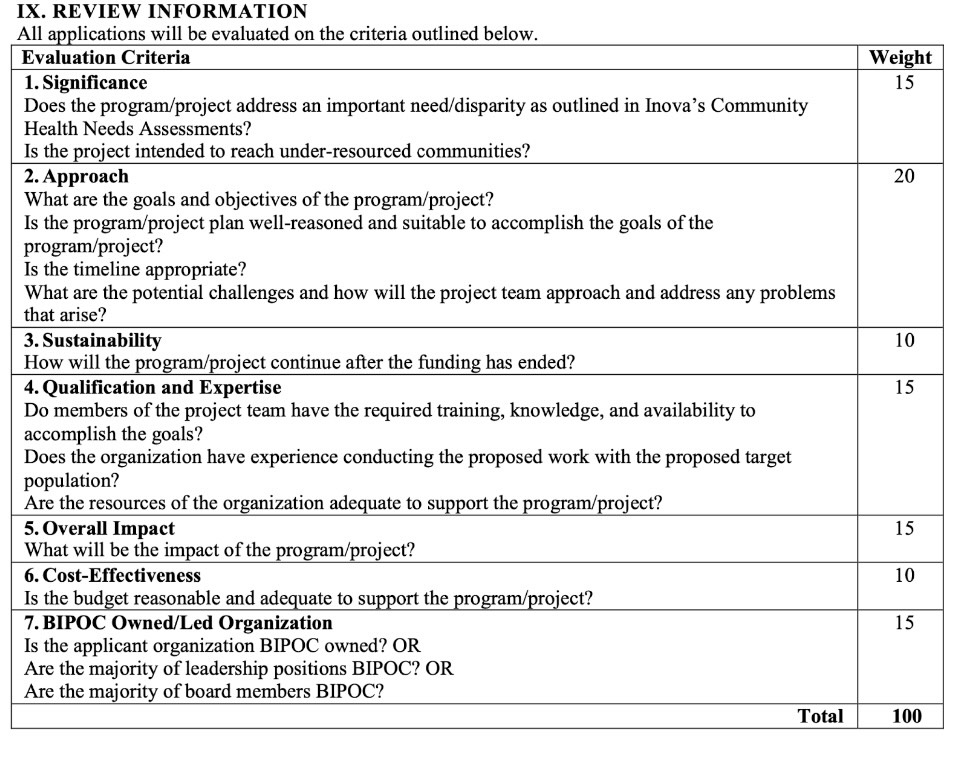
“Inova does not support programs or projects that discriminate on the basis of gender, race, color, religion, or sexual orientation,” the document states.
Subsequent grant programs, including one launched in March, say they consider “BIPOC” ownership but do not provide a detailed scoring breakdown.
While not technically a case of contracting, the grant recipients are part of the public health infrastructure of the greater Washington, D.C., area. Past winners include primary care providers, dentists, and mental health nonprofits that work with underprivileged patients, many of them below the poverty line.
“These investments have meaningfully supported the ability of our non-profit partners to address community health issues,” an Inova spokeswoman, Renee Brohard, told the Free Beacon. She declined to comment on whether the weighting scheme from 2021 is still in use.
Fifteen out of 100 points might not sound like much in absolute terms. But in the context of a competitive bidding process, it can easily swing a grant or contract to a less efficient firm.
Under the point system adopted by JPS Health, for example, “a typical firm could sell the same good up to 60 percent cheaper and still lose a contract to a minority, woman, or veteran-owned firm,” said Glock, who reviewed several of the health system’s scoresheets at the Free Beacon‘s request.
That leg-up is extreme relative to other minority contracting programs, Glock added, where the extra cost is more like 10 percent.
These preferences pose legal as well as economic issues. While private grantmakers like Inova can, in most cases, dole out money based on race, minority contracting is only allowed as a remedial measure—that is, to offset the effects of past discrimination in public procurement. That means governments must commission “disparity studies”—expert reports on the obstacles faced by minority businesses in an area—before they engage in race-conscious contracting.
Tarrant County does not appear to have conducted such a study, unlike some of its adjacent districts. And while the county’s procurement policies do encourage the use of “historically underutilized businesses,” they also state that this should be done through “race, ethnic and gender neutral means.”
“That certainly raises questions about what exactly Tarrant County is doing,” said Dan Morenoff, the executive director of the American Civil Rights Project, a conservative public interest law firm. If the county’s health system “is discriminating based on race without a study—as its pitch materials and scorecard seem to indicate, even if they now deny it—that would make it very hard for the policy to pass constitutional muster.”
JPS Health said its procurement procedures were “consistent with the law” and parallel the policies of “other local governmental entities.”
Contracting is far from the only area in which medical bureaucracies have injected race, and far from the most explosive. Many Americans were outraged when, in 2022, some states and hospitals systems gave minorities extra points when allocating COVID drugs, using score sheets like the ones at JPS Health to determine which patients would be eligible for scarce therapies. More recently, the National Institutes for Health has faced blowback for distributing research grants based on race.
These controversies come at a moment of legal precarity for racial preferences. Though minority contracting hasn’t yet been struck down, the Supreme Court’s ban on affirmative action in college admissions has amplified scrutiny on, and challenges to, all sorts of race-conscious initiatives, including one run by the Small Business Administration.
That initiative, the 8(a) Business Development Program, funnels billions of contracting dollars to “disadvantaged” firms. A district judge ruled last year that companies could not automatically qualify for the program based on race, citing the Supreme Court’s decision.
“For public hospitals, minority contracting preferences could run afoul of the legal requirement that public entities give equal protection of the law to all races,” Glock said. In the wake of the Supreme Court’s decision, preferences like Tarrant County’s “are more legally vulnerable than ever.”
Original News Source – Washington Free Beacon
Running For Office? Conservative Campaign Management – Election Day Strategies!